Medicine Discussion
MEDICINE
BIMONTHLY ONLINE
ASSESSMENT -1
This is to discuss , understand and review clinical scenarios so as to improve my clinical competency via online e-logging clinical cases
The cases have been shared after patient / Guardian signed informed consent
S.Kavya , 8th sem
Roll no 121
1) Pulmonology
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Evolution of symptomatology

Anatomical location - lungs
Primary etiology - usage of chulha since 20years, might be due to its chronic usage
And possible etiology - Any Exposure to the causative allergen in her paddy field since she has been having yearly episode of SOB in the month January every year - it is same period of time (winter) paddy is grown
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
2Ans)Head end elevation

MOA;
.improves oxygenation
.decreases incidence VAP
.increases hemodynamic performance
.increases end expiratory lung volume
.decreases incidence of aspiration
Indication:
.head injury
.meningitis
.pneumonia
oxygen inhalation to maintain spo2
Bipap:non invasive method

MOA :assist ventilation by delivering positive expiratory and inspiratory pressure with out need for ET incubation
3) What could be the causes for her current acute exacerbation?
Could be due to any infection

https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2645331/
4. Could the ATT have affected her symptoms? If so how?
Yes, ATT affected her symptoms
rifampicin - causes swelling and streptomycin is a Nephrotoxic - Renal damge -lead to electrolyte imbalance
5.What could be the causes for her electrolyte imbalance?
ATT could have caused renal damage which lead to her electrolyte imbalance
Neurology
(A)
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Timeline of patient symptomatology:
2009 (12 years ago): Started drinking alcohol
||
2019 (2 years ago): Diagnosed with Diabetes Mellitus, prescribed oral hypoglycemics
||
2020 (1 year ago): Has an episode of seizures (most likely GTCS)
||
January 2021 (4months ago): Has another seizure episode (most likely GTCS)- following cessation of alcohol for 24 hours. Starts drinking again after seizure subsides
||
Monday, May 10, 2021: Last alcohol intake, around 1 bottle. Starts having general body pains at night.
||
Tuesday, May 11, 2021: Decreased food intake. Starts talking and laughing to himself. Unable to lift himself off the bed, help required.
Conscious, but non coherent. Disoriented to time, person, place.
||
Saturday, May 15, 2021: Is admitted to a tertiary care hospital for alcohol withdrawal symptoms, and is treated for the same.
Anatomical localisation of problem: hippocampus and frontal lobe.
Primary etiology of patient's problem: Chronic Alcoholism
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
1) IVF - NS and RL
MOA -maintains blood volume and electrolytes in the body and also provides Glucose to the body
indications: dehydration, hypovolemic shock, to restore fluids after burns.
2) inj. Thiamine : MOA : vitamin B1, Provides energy in deficiency conditions
Indications:
* deficient conditions, wernickes encephalopathy, Diarrhoea, ulcerative colitis.
3) inj. Lorazepam _ Benzodiazepine
MOA : enhances the inhibitory effects of GABA - INHIBITORY NEUROTRANSMITTER.
indications; * anxiety disorders, panic disorders, seizures, pre operative sedation.
4) tab. Pregabalin _anticonvulsant
MOA: binds to alpha 2 voltage gated calcium channels in cns and inhibits release of excitatory neurotransmitters
indications ;
*partial seizures
*nerve pain
*fibromyalgia
5) inj. HAI - insulin
#MOA : reduces blood glucose levels by increasing peripheral uptake of glucose by muscle.
Indications:
*Type 1 Dm
*uncontrollable type 2 DM
* DKA
6) Grbs; test to identify blood glucose levels
7) lactulose : artificial Dischaaride
indications:
* chronic constipation
*hepatic encephalopathy
8) inj. Kcl _ electrolytes
MOA; prevents low blood levels of potassium
indications ;
* hypokalemia
To correct deficiency, vomiting, weakness
9) syrup potchlor- contains potassium chloride, and prevents low levels of potassium in the body
indications;
*deficiency of potassium
* electrolyte imbalance
3) Why have neurological symptoms appeared this time, that were absent during withdrawal earlier? What could be a possible cause for this?

4) What is the reason for giving thiamine in this patient?

Thiamine is necessary to provide energy to the CNS, helps in conduction of nerve signals.

5) What is the probable reason for kidney injury in this patient?
Creatinine and urea levels are very high, it denotes an acute onset- Acute Renal Failure.
It could be due to dehydration which lead to Acute tubular necrosis
6). What is the probable cause for the normocytic anemia?
causes:
a. Increased oxidative stress and inflammation, leading to hemolysis of the RBCs

b. Decreased bone marrow production of RBCs, due to EPO deficiency owing to kidney failure
c. Loss of blood through chronic foot ulcer
7) Could chronic alcoholism have aggravated the foot ulcer formation? If yes, how and why?
Yes, as alcoholism itself can cause peripheral neuropathy ,which along with Diabetic neuropathy, can lead to a non-healing foot ulcer.
(B)
https://kausalyavarma.Complete regarding the case are in the mentioned link above
Questions-
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?

Anatomical location - right inferior cerebellar hemisphere
Primary etiology - Hypertension
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
1) Tab. Vertin- Betahistine
MOA: agonist of H1 receptor and antagonist of H3 receptor , improve the microcirculation of inner ear
indications:vertigo, tinnitus
2) inj.zofer- ondansetron - ANTIEMETIC
MOA: binds to 5 HT3 receptor and thus inhibits the binding of serotonin to it .
#indications: nausea and vomiting due to any cause
3) Tab. Ecosprin- antiplatelet drug
MOA : low dose Aspirin prevents blood clot formation by inhibiting the action of COX enzyme
# indications;
*stroke
* angina
* heart attack
4) Tab. Atorvastatin- statins
MOA :HMG CO-A reductase inhibitor, thus decrease cholesterol production in liver.
indications;
*MI
*STROKE
*ANGINA
5) BP monitoring
6) Tab. Clopidogrel- antiplatelet drug
MOA: inhibits the binding of ADP to platelet P2Y12 receptor and subsequent ADP mediated activation of
GP2b/3a complex, action which is irreversible.
#Indications:
*during PCI
*ACS
*Prevention of Thrombiembolism
*carotid artery stenosis
7) inj. Thiamine- vitamin B1
MOA:combines with ATP to produce thiamine Diphosphate , coenzyme in carb metabolism, utilization of hexose in HMP pathway.
#Indications;
*to correct deficiency
*beri beri
*neuritis
8) Tab. Mvt. - vitamins and minerals
Indication : to correct deficiency and anemia
3) Did the patients history of denovo HTN contribute to his current condition?
Yes
Decreased blood supply to that area - infarction - cerebellar infarct
Hypertension - Atherosclerosis - Ruptures- Stroke- Cerebellar infarcts

4)Does the patients history of alcoholism make him more susceptible to ischaemic or haemorrhagic type of stroke?
Alcohol is a risk factor for atherosclerosis which causes - Ischemia - Ischemic stroke

(C)
http://bejugamomnivasguptha.Complete details regarding the case are in the mentioned link above
Questions:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?

For radiating pain along left upper limb is due to cervical spondylitis
2) What are the reasons for recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
Could be due to inadequate intake
Could be inherited also
3) What are the changes seen in ECG in case of hypokalemia and associated symptoms?
Earliest change sen in ECG is decreased T wave amplitude
ST depression, T wave inversion, flat
Prolonged PR
Uwaves

D) Link to patient details:
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
QUESTIONS
1.Is there any relationship between occurrence of seizure to brain stroke. If yes what is the mechanism behind it?
seizures after ischaemic strokes. An increase in intracellular Ca2+ and Na+ with a resultant lower threshold for depolarisation, glutamate excitotoxicity, hypoxia, metabolic dysfunction, global hypoperfusion, and hyperperfusion injury
Seizures after haemorrhagic strokes are thought to be attributable to irritation due to (hemosideri. Deposits)caused by products of blood metabolism
Late onset seizures are associated with the persistent changes in neuronal excitability and gliotic scarring is most probably the underlying cause.


2. In the previous episodes of seizures, patient didn't loose his consciousness but in the recent episode he lost his consciousness what might be the reason?
Initially the patient might have had Simple partial seizures (no loss of consciousness) and might have progressed to Generalised Tonic Clonic seizures (loss of consciousness)

Loc - loss of consciousness
E) Link to patient details:
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
Questions: 1) What could have been the reason for this patient to develop ataxia in the past 1 year?
The patient has minor unattended head injuries in the past 1 yr. Accoding to the CT scan, the patient has cerebral haemorrhage in the frontal lobe causing probably for the occurrence of Frontal lobe ataxia

2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
The patient has minor unattended head injuries. During the course of time the minor hemorrhages if present should have been cured on their own. But the patient is a chronic alcholic. This might have hindered the process of healing or might have stopped the healing rendering it to grow further more into 13 mm sized hemorrhages occupying Frontal Parietal and Temporal lobes
Liver damage due to too much alcohol can stop the liver from synthesis of coagulants this may be the reason for his IC bleed
F) Link to patient details:
Questions
1.Does the patient's history of road traffic accident have any role in his present condition?
Yes
2.What are warning signs of CVA?
Weakness or numbness of the face, arm or leg, usually on one side of the body
Trouble speaking or understanding
Problems with vision, such as dimness or loss of vision in one or both eyes
Dizziness or problems with balance or coordination
Problems with movement or walking
Fainting or seizure
Severe headaches with no known cause, especially if they happen suddenly

3.What is the drug rationale in CVA
Mannitol-
Because of its osmotic effect, mannitol is assumed to decrease cerebral edema. Mannitol might improve cerebral perfusion by decreasing viscosity, and as a free-radical scavenger, it might act as a neuroprotectant.
Ecospirin
For the prevention of heart attack, stroke, heart conditions such as stable or unstable angina (chest pain) due to a blood clot.
New insights into the mechanisms of action of aspirin and its use in the prevention and treatment of arterial and venous thromboembolism
Atrovas-Atorva
40 Tablet belongs to a group of medicines called statins. It is used to lower cholesterol and to reduce the risk of heart diseases. Cholesterol is a fatty substance that builds up in your blood vessels and causes narrowing, which may lead to a heart attack or stroke.
Rt feed RT feed is a nursing procedure to provide nutrition to those people who are either unable to obtain nutrition by mouth or are not in a state to swallow the food safely.
Insulin:
Hypoglycemia can cause focal neurologic signs that mimic stroke and can itself lead to brain injury..
Therefore, prompt measurement and normalization of serum glucose concentration is important. Subcutaneous insulin is administered to keep glucose less than 180 mg/dL.
Antipyretics
Increased body temperature in the setting of acute ischemic stroke has been associated with poor neurologic outcome, possibly due to increased metabolic demands, enhanced release of neurotransmitters, and increased free radical production.
Maintaining normothermia might improve the prognosis of patients with severe events using antipyretic medications and cooling devices. Antipyretic therapy is indicated for temperatures above 37.5 °C.
Increased body temperature in the setting of acute ischemic stroke has been associated with poor neurologic outcome, possibly due to increased metabolic demands, enhanced release of neurotransmitters, and increased free radical production.
Maintaining normothermia might improve the prognosis of patients with severe events using antipyretic medications and cooling devices. Antipyretic therapy is indicated for temperatures above 37.5 °C.
Thrombolysis
Intravenous administration of alteplase is the only US Food and Drug Administration (FDA)-approved medical therapy for treatment of patients with acute ischemic stroke
Intravenous administration of alteplase is the only US Food and Drug Administration (FDA)-approved medical therapy for treatment of patients with acute ischemic stroke
4. Does alcohol has any role in his attack?
When the patient met with an accident there might be cranial damage which was unnoticed.
If so his occasional drinking may or may not have hindered the process of the minor hemorrhages getting healed and might have caused this condition
But since the patient is not a chronic alcoholic and so Alcohol might not have played any role.
Therefore it cannot be evaluated without further details
5.Does his lipid profile has any role for his attack??
The inverse relationship between serum HDL-C and stroke risk . When taken together it seems clear that higher baseline levels of serum HDL-C lower the risk of subsequent ischemic stroke.
(G)
Complete details regarding the case are in the mentioned link abovehttps://amishajaiswal03eloggm.
1)What is myelopathy hand ?
a)There is loss of power of adduction and extension of the ulnar two or three fingers and an inability to grip and release rapidly with these fingers. These changes have been termed "myelopathy hand" and appear to be due to pyramidal tract involvement.

2) what is Finger escape
Wartenberg's sign is a neurological sign consisting of involuntary abduction of the fifth (little) finger, caused by unopposed action of the extensor digiti minimi. . This finding of weak finger adduction in cervical myelopathy is also called the "finger escape sign".

3) what is Hoffman's sign
Hoffman's sign is a test used to examine the reflexes of the upper extremities. This test is a quick, equipment-free way to test for the possible existence of spinal cord compression from a lesion on the spinal cord or another underlying nerve condition

(H)
Complete details regarding the case are in the mentioned link above
https://neerajareddysingur.
Possible questions:
1) What can be the cause of her condition ?
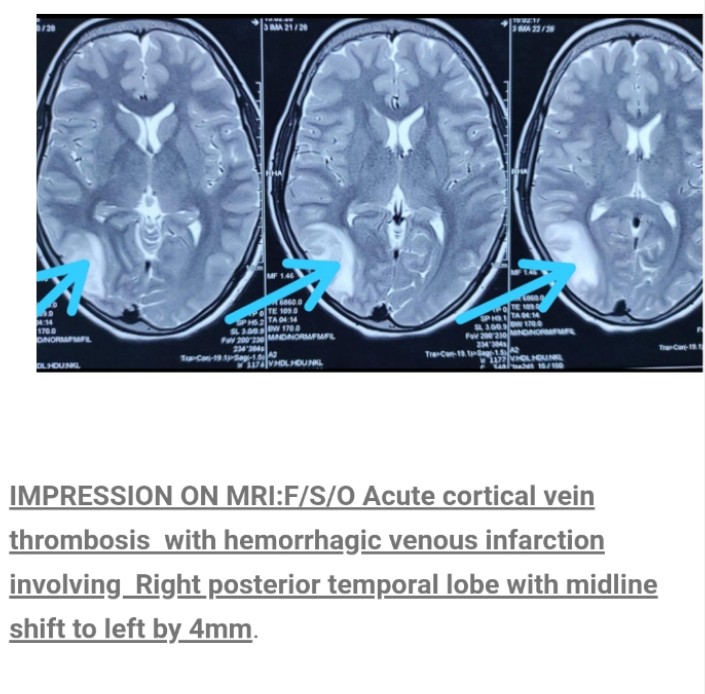
2) What are the risk factors for cortical vein thrombosis?
Infections:
Meningitis, otitis,mastoiditis
Prothrombotic states:
Pregnancy, puerperium,antithrombin deficiency proteinc and protein s deficiency,Hormone replacement therapy.
Mechanical:
Head trauma,lumbar puncture
Inflammatory:
SLE,sarcoidosis,Inflammatory bowel disease.
Malignancy.
Dehydration
Nephrotic syndrome
Drugs:
Oral contraceptives,steroids,Inhibitors of angiogenesis
Chemotherapy:Cyclosporine and l asparginase
Hematological:
Myeloproliferative Malignancies
Primary and secondary polycythemia
Intracranial :
Dural fistula,
venous anomalies
Vasculitis:
Behcets disease wegeners granulomatosis
3)There was seizure free period in between but again sudden episode of GTCS why?resolved spontaneously why?
Seizures are resolved and seizure free period got achieved after medical intervention but sudden episode of seizure was may be due to any persistence of excitable foci by abnormal firing of neurons.
4) What drug was used in suspicion of cortical venous sinus thrombosis?
Anticoagulants are used for the prevention of harmful blood clots.
Clexane ( enoxaparin) low molecular weight heparin binds and potentiates antithrombin three a serine protease Inhibitor to form complex and irreversibly inactivates factor xa.
3) Cardiology
(A)
1.What is the difference btw heart failure with preserved ejection fraction and with reduced ejection fraction ?


-
2.Why haven't we done pericardiocenetis in this pateint?
ANS;
Pericardiocentesis is done when the pericardial effusion is not resolving on its own . Here the pericardial fluid which has accumulated was resolving on itw own , at the time of admission it was 2.4mm and when discharged it was 1.9 mm . Therefore we did not do pericardiocentesis in this pt.
3.What are the risk factors for development of heart failure in the patient?
ANS: IN THIS PATIENT:
NON MODIFICABLE:
age
gender
MODIFIABLE:
hypertension
smoking
type 2 diabetes .
kidney disease.
4.What could be the cause for hypotension in this patient?
The pt. was anemic with Hb of 8gm/dl . One of the severe complication of anemia is tissue hypoxia which further lead to hypotension.
(B)
Link to patient details:
https://muskaangoyal.blogspot.
1.What are the possible causes for heart failure in this patient?
ANS:
obesity
alcohol
diabetes
hypertension
2.what is the reason for anemia in this case?
Alcoholics frequently have defective red blood cells that are destroyed prematurely, possibly resulting in anemia.

3.What is the reason for blebs and non healing ulcer in the legs of this patient?
The pt. had recurrent blebs and ulcer on lower limbs (foot). This is due to Type to diabetes mellitus.
Diabetic foot ulcers generally arise as a result of poor circulation in the foot region. While high blood sugar levels and nerve damage or even wounds in the feet may result in foot ulcers in many cases.
In cases of poor circulation of blood, the foot ulcers take quite a bit of time to heal as the blood efficiency in the foot region is at a low level. Furthermore, many develop a bit of reduced sensation on the feet as a result of nerve damage or more.
There are many risk factors that may lead to foot ulcers at the end.
Poor quality or fitting of the footwear.
Unhygienic appearance of foot.
Improper care of the nails of the toe.
Heavy intake of alcohols and tobacco.
Obesity and Weight-related
Complication arising from Diabetes like eye problems, kidney problems and more.
Although aging or old age can also be counted among them.
4. What sequence of stages of diabetes has been noted in this patient?
alcohol consumption lead to obesity which caused impaired glucose tolerance - Diabetes mellitus -microvascular complications like triopathy and diabetic foot ulcer
macrovascular complications like coronary artery disease , coronary vascular disease and peripheral vascular disease.
C)
Link to patient details:
https://preityarlagadda.
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans:.

the anatomical site is BLOOD VESSELS;
ETIOLOGY:
The physical stress of hypertension on the arterial wall also results in the aggravation and acceleration of atherosclerosis, particularly of the coronary and cerebral vessels. Moreover, hypertension appears to increase the susceptibility of the small and large arteries to atherosclerosis.
The most likely cause of arterial thrombosis is artery due to atherosclerosis. Atherosclerosis occurs when a person has a buildup of plaque on the walls of their arteries. The arteries then begin to narrow and harden, which increases a person's risk of developing arterial thrombosis.
2) What are mechanism of action, indication and efficacy over placebo of each of the pharmacological and non pharmacological interventions used for this patient?
Ans: PHARMACOLOGICAL INTERVENTIONS
1. TAB. Dytor
mechanism: Through its action in antagonizing the effect of aldosterone, spironolactone inhibits the exchange of sodium for potassium in the distal renal tubule and helps to prevent potassium loss.
2. TAB. Acitrom
mechanism: Acenocoumarol inhibits the action of an enzyme Vitamin K-epoxide reductase which is required for regeneration and maintaining levels of vitamin K required for blood clotting
3. TAB. Cardivas
mechanism:Carvedilol works by blocking the action of certain natural substances in your body, such as epinephrine, on the heart and blood vessels. This effect lowers your heart rate, blood pressure, and strain on your heart. Carvedilol belongs to a class of drugs known as alpha and beta-blockers.
4. INJ. HAI S/C
MECHANISM:Regulates glucose metabolism
Insulin and its analogues lower blood glucose by stimulating peripheral glucose uptake, especially by skeletal muscle and fat, and by inhibiting hepatic glucose production; insulin inhibits lipolysis and proteolysis and enhances protein synthesis; targets include skeletal muscle, liver, and adipose tissue
5.TAB. Digoxin
mechanism:
Digoxin has two principal mechanisms of action which are selectively employed depending on the indication:
Positive Ionotropic: It increases the force of contraction of the heart by reversibly inhibiting the activity of the myocardial Na-K ATPase pump,
an enzyme that controls the movement of ions into the heart
6. Hypoglycemia symptoms explained
7. Watch for any bleeding manifestations like Petechiae, Bleeding gums.
8. APTT and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to make sure that the drug is producing the desired effect.
3) What is the pathogenesis of renal involvement due to heart failure (cardio renal syndrome)? Which type of cardio renal syndrome is this patient?
Ans:

Cardiorenal syndrome type 4 is seen in this patient.
4) What are the risk factors for atherosclerosis in this patient?
Ans: effect of hypertention
They can also impair blood vessels' ability to relax and may stimulate the growth of smooth muscle cells inside arteries. All these changes can contribute to the artery-clogging process known as atherosclerosis.
5) Why was the patient asked to get those APTT, INR tests for review?
Ans: APTT and INR are ordered on a regular basis when a person is taking the anticoagulant drug warfarin to make sure that the drug is producing the desired effect.
Here, an INR of 3-4.5 is recommended. Warfarin should be started in conjunction with heparin or low molecular weight heparin when the diagnosis of venous thromboembolism is confirmed, although local protocols may vary in their starting doses and titration schedule.
D)



E)
F)
Link to patient details:
4) Gastroenterology (& Pulmonology)





5) Nephrology (and Urology)


6) Infectious Disease (HI virus, Mycobacteria, Gastroenterology, Pulmonology)


7) Infectious disease and Hepatology:







Comments
Post a Comment